Company & Product
ASTRO 2019 Highlights
We had an excellent meeting in the windy city! ASTRO 2019 was filled with groundbreaking research, collaborative learning, and interesting new...
A realistic inquiry into the clinical realities of adaptive radiotherapy, examining the pitfalls and promise of this game-changing treatment approach.
In some form or fashion, we’re all aware of what adaptive radiotherapy (ART) is. You’ve probably treated a head and neck patient whose tumor responds quickly to radiation. Or a patient that loses weight during their course and requires a replan. But there’s more to it than the occasional mid-course replan.
If it’s a trendy topic now, it’s not because it’s new to the scene. Making changes to plans during a course of treatment has been common for decades, but now it’s back in the spotlight (*ahem*, FLASH radiotherapy). The renewed swell of interest and activity is due to developments in online adaptive treatments, in which plan adjustments are made in real time as the patient is on the table.
But in radiation oncology, there’s no free lunch, and mid-course treatment changes come at a cost. In the most basic offline case, sufficient time is needed to perform a replan, which might include a new image set, new contours, MD input, physics QA, etc. For more complicated online approaches, sophisticated tools and advanced workflows are required for more frequent iterations, involving additional on-demand staffing. With all of this in mind, is the hype surrounding the renewed adaptive movement warranted?
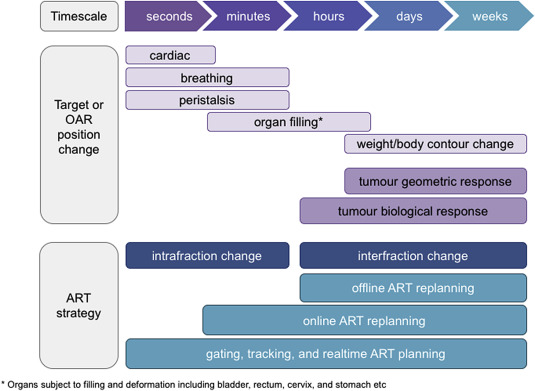
Timelines and implementation approaches for adaptive radiotherapy. Credit: A. Hunt, et al., Adaptive Radiotherapy Enabled by MR Guidance
The Basics
In talking about this subject of adaptive radiotherapy, it’s worth pointing out it’s a rather broad topic that encompasses various timelines and approaches. But there’s a common motivation behind all permutations: the desire to monitor radiotherapy plans for clinical acceptability and modify the plan as necessary with the goal of improving clinical outcomes.
Given the demographic stratification of this blog’s audience, you’re coming in with some basic knowledge of this topic. But for completeness, let’s first establish some basic points:
What is adaptive radiotherapy?
This is a treatment approach that tailors the radiation plan to suit the anatomical changes of a tumor and surrounding tissues throughout the therapy course. The goal of these modifications is to optimize the overall accuracy of the treatment delivery.
This differs from traditional radiotherapy in which, typically, a single plan is generated based on a pre-treatment CT. Though minor alignment adjustments may be applied in response to daily imaging, replanning is typically not justified throughout the course of treatment. As a result of this, we accept some degree of uncertainty on individual fractions. But with appropriate margins and long fractionation schemes, the idea is that these variations average to something that looks like the original treatment plan.
How is offline different from online?
The central component that distinguishes offline and online versions of these changes in treatment is the timeline. When clinical necessity requires a replan, but the new plan is generated between fractions, the adaptation is offline. Online suggests a retooling—which can include a new image and structure set, calculations, QA, etc.—that takes place while the patient is on the table.
What can we gain from this type of therapy?
The full potential of adaptive radiotherapy is yet undiscovered and unrealized. Presently, there are few publications that validate our collective hunch that there is potential here. But intuitively, there are a few advantages that this treatment approaches can offer:
Reasons for Caution
Adaptive RT paints a dazzling picture of personalized cancer treatment fit for a new era in radiation oncology. But while the promises are music to any oncologist's ears, this treatment approach is expensive, requires additional resources and staffing, and workflows are yet unrefined.
This naturally begs the question: do we have robust clinical data to justify the additional cost? Are we overlooking the sustainability of this approach in the face of limited healthcare resources? Volatility in the MR-linac market, highlighted by the struggles and subsequent acquisition of ViewRay (a surprise given its prominence as a manufacturer of MR-guided adaptive systems), raises concerns about the sustainability of this market segment and prompts a fair appraisal of the long-term viability of this type of intervention.
Data Challenging Our Optimism
Some of the data being published on adaptive schema indicate that improved dosimetric conformality and escalation do not necessarily lead to advantageous clinical outcomes.
In a 2021 abstract in the Journal of Clinical Oncology investigating the impact of weekly adaptation of head and neck IMRT patients, Maulik, et. monitored doses to the parotids. If anatomical changes resulted in a dose increase to the parotids above 2%, a replan was attempted in an effort to reduce the dose to the parotids while maintaining PTV coverage such that the mean dose to the parotids was maintained. They were unable to show that mid-course intervention to maintain parotid dose improved various quality of life indicators. Their conclusion posits that, “The benefits of adaptive replanning strategies based on weekly evaluation, binary thresholds, and standard planning procedures is doubtful.”
A phase 3 randomized clinical trial published in 2023 in JAMA Oncology took a similar approach. The study also investigated weekly replanning for impact on the frequency of xerostomia for a cohort of locally advanced oropharyngeal cancer patients receiving IMRT treatments. While excretory function (as measured using Tc-99m scintigraphy) improved slightly in the adaptive arm, other measures, including their primary salivary flow (xerostomia) endpoint, did not. In their conclusion, they state, “This randomized clinical trial did not demonstrate a benefit of ART in decreasing xerostomia compared with standard IMRT.”
It’s important to note that these two studies re-evaluated patients for change on a weekly basis, not daily or PRN. But both studies made regular efforts to adapt mid-course and still did not demonstrate any benefit in terms of reducing xerostomia.
Another study in the Journal of Thoracic Oncology focused on the role of dose escalation using mid-treatment PET/CT guided adaptive treatments for locally advanced non-small cell lung cancer. Despite a median prescription dose of 71Gy in the adaptive arm (versus 60Gy in the standard arm), there were “no significant differences in overall survival, progression free survival, or lung cancer specific survival between the two arms.”
Similar to the parotid studies, this phase II lung cancer trial was not reevaluated on a daily basis, so a direct comparison to daily changes may not be completely appropriate. But given that these attempts to escalate dose or spare critical tissues didn’t result in improved clinical outcomes, is there anything to suggest that adapting on a daily basis will provide better results?
The Cost of Admission
With any ART regimen, whether plan changes are implemented once per course, weekly, or daily, additional work is involved in creating a new plan. For even simple cases, that requires a new image set, newly contoured structures, a replan, and thorough review. As Malik, et al. concluded in their Journal of Clinical Oncology abstract, “The average time required for each step in the planning process was comparable for both the initial planning workflow and adaptive replanning process.” That is to say, replanning isn’t any less time-consuming than designing the original treatment plan. For busy departments, additional planning for existing patients can strain existing resources.
What does this mean in practical terms for clinics looking to understand the cost of adaptive RT? An Advanced Radiation Oncology study published in 2023 determined that, based on data from 415 treatment fractions, an additional 16 minutes are needed for each adaptive fraction. When accounting for staff salaries for the individuals present for the adaptive sessions, the average cost per CT-based adaptive fraction was calculated to be $103.58.
Another study from Washington University suggests the appointment times for ART, depending on technique and site, are sometimes longer and may require more than just 16 minutes. For their adaptive gated pancreas SBRT, for example, their treatment time slot is 80 minutes. Even if we were to accept the estimated CT-based adaptive costs, this could amount to thousands of dollars in additional burden per patient, depending on the number of adapted fractions per course.
But these are just additional staffing costs, which may be the smallest piece of the proverbial pie. Getting an online program jumpstarted requires specialty treatment machines and/or dedicated hardware. Many adaptive programs utilize MR linacs to exploit the improved soft tissue contrast the imaging modality offers, which is an excellent therapy adjunct for many abdominal targets. These machines are markedly more expensive than CT-based linacs. The list price for an MRIdian linac was estimated to be $7.8M according to a 2020 cost comparison of CT-guided versus MR-guided SBRT. With special considerations (and additional budgeting) for MR vault construction, a new MR linac project can soar well above $10M.
Check Please
But who pays for it? Are patients responsible for any, or all, of the additional replans? Does the clinic absorb the cost? Currently there are no CPT codes associated with adaptive RT, so departments that offer this service cannot explicitly bill for it. That doesn’t mean that they can’t bill something. But at the moment, standard practices in this regard have not yet been codified.
According to radiation oncologist Percy Lee, MD, “Billing for adaptive is a gray zone at this point in time. The additional work that is associated with online adaptive should be accounted for somehow via reimbursement. But presently, there is no clear path to account for this work in the current payment model and that must change for this new technology, which inherently requires more resources to succeed. There’s probably a right way and a wrong way to bill for it, but everyone is approaching it differently. We’re trying to be conscientious of billing only when the work is medically necessary and when it feels like we’re doing the right thing for the patient.”
He goes on to comment on the market for adaptive RT, “I also agree that we need to continue data collection to show the clinical benefits of all this additional work. And after all, it’s completely fair to be skeptical of human behavior when driven by financial incentives. Are people installing these perhaps in part because of some local competition to have the most cutting-edge resources? As an industry, we need to be mindful that adaptive radiotherapy isn't being oversold for reasons beyond genuine improvements in patient care.”
Adaptive is Staff-Intensive, Cumbersome
As alluded to in the financial feasibility study referenced above, the staffing resource demands are elevated for adaptive treatments. Their calculations of additional cost burden factored in on-demand resources of one physician, one physicist, one dosimetrist, and two therapists. According to Lee, “It’s very staff-intensive. In the beginning, we were very focused on making adaptive radiotherapy more efficient. But the reality is, we’re struggling with staffing in radiation oncology at this moment in time.”
Even with proper staffing, workflows can be complicated and cumbersome, which results in longer patient appointment times. In a 2021 review article from Frontiers in Oncology, the authors state, “To date, the clinical workflow burden of ART is one of the major reasons limiting its widespread acceptance.”
But if adaptive teams are able to fit contouring, replanning, and QA into a mere 15-20 additional minutes—when it takes multiple days of passive work under normal circumstances—is that not efficient enough? AI contouring has been a boon for fast contouring times, and as computer power scales, automation matures, and we get a better sense of the general needs for adaptive throughput, this intense workflow will likely continue to improve in the future.
The Baby in the Bath Water
With so much to support the devil’s advocate point of view regarding adaptive, is our intuitive clinical gut feeling that this approach makes sense just…wrong?
Because adaptive radiotherapy is in its infancy, data of any kind to support this treatment approach is scarce. “Without data, there is a reason to be skeptical. But skepticism should have its limits: adaptive machines have not been around for long enough for many large pools of data to be accumulated,” says Alex Price, PhD, medical physicist at University Hospitals in Cleveland, OH.
In a statement encouraging patience, Price says, “If it makes sense, even if slightly impractical at first, we can make that work and improve efficiency in the future. Remember, in the early days of IMRT we were still imaging cervical patients with kV/kV films. Clearly we see the value of CBCT now, but there were likely skeptics of CBCT when it arrived on the scene.”
While there are many cost, staffing, and workflow considerations that challenge widespread adoption of ART, there are some promising studies that suggest we may be at the forefront of something transformative.
Adaptive Radiotherapy Shows Potential
Michael Chuong, MD agrees with Price about the need for more studies. “As an oncologist, I don’t need data to intuitively understand that sparing normal tissue and escalating target dose is a good idea. But yes, we need more clinical trials to really understand the impact on patients,” he says. He and his team at Miami Cancer Institute have taken it upon themselves to produce this data. In a study published in 2022 in Frontiers in Oncology, early results of their ablative stereotactic magnetic resonance image-guided adaptive radiation therapy (A-SMART) program showed very minimal toxicity (4.8% acute and late grade 3 toxicities) and encouraging local control (45.5% 2-year overall survival).
Chuong followed that study up with a multi-institutional phase II trial that evaluated the safety and efficacy of A-SMART for pancreatic cancer. The results of the phase II trial indicate promising overall survival rates and minimal severe (late grade ≥ 3 toxicity) side effects.
There is additional data showing reduced toxicity using tighter margins. In the non-adaptive phase 3 MIRAGE trial, the reduction of planning margins from 4mm to 2mm in SBRT prostate delivery. The trial data shows significantly lower incidence of acute grade 2 or greater GU toxicity with MRI guidance and 2mm margins (24.4% vs 43.4%).
There is a growing body of evidence supporting the use of MR-guided ART for the treatment of inoperable pancreatic cancer. In a 2019 study published in Cancer Medicine evaluating MR-guided ART comparing dose escalation (BED10>70Gy) to standard dose (BED10<70Gy), the data showed improvement in 2-year overall survival for the dose escalation arm.
As Price puts it, “Where we’ll make gains in adaptive is improving the therapeutic ratio. If we don’t have room to make a clinically significant difference in the prescription doses to targets, we’re going to be limited. Is the additional sparing making a difference for the OARs? Maybe, but it’s going to be challenging to resolve, or it will only make a minor difference. We should probably be more focused on dose escalation to go for tumor control,” he says.
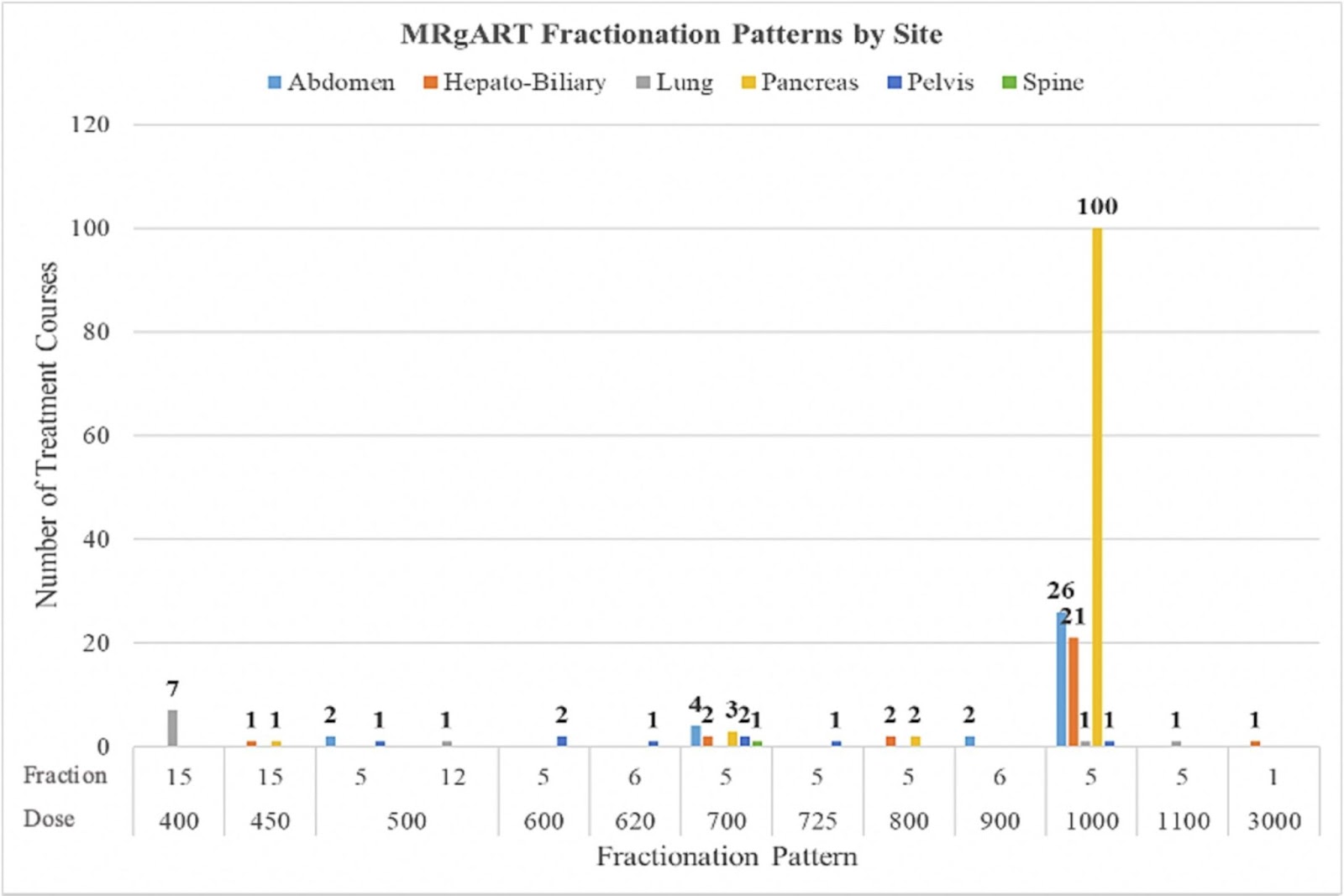
Institutions employing this form of treatment seem to share an understanding that the pancreas stands to derive significant benefits from it. The practice data from Washington University shows that pancreas is an important treatment site for their ART program. A large majority of their MRgRT volume consists of pancreas cases, where they’ve been exploiting the potential for dose escalation to improve outcomes for these patients.
Distribution of MRgRT Fractionation Patterns by site at Washington University as published by Price, et al.
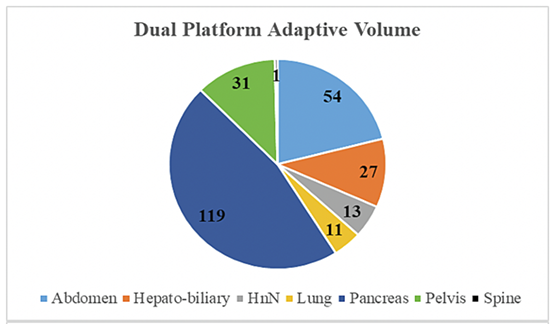
Distribution of sites treated with adaptive radiotherapy (accounting for both CT and MR platforms) at Washington University according to the 2023 review of its institutional experience as published in Clinical and Translational Radiation Oncology.
Beyond Online Adaptive
This method is new and hasn’t accrued a large amount of incontrovertible evidence to establish clinical necessity, and there are some hurdles to wider adoption. Despite these roadblocks, we may see in the coming years that adaptive radiotherapy—both online and offline— has more than just potential.
As automation and AI continue to improve workflows, bringing new tools to streamline contouring, planning, and QA, offline adaptive could become a more accessible option for those clinics that cannot commit to more in-depth and rigorous online routines. “Making offline adaptive easier and faster would be of particular benefit to our field, since it is many times not triggered until the anatomic changes are especially large and where in retrospective treatment plan modification ideally should have been done sooner,” says Chuong.
Also, committing to an MR-linac or specialty adaptive machine doesn’t limit departments to a single treatment approach. The sites that opt for treatment machines capable of online adaptive find that they are more than one trick ponies. Many sites are leveraging improved on-board imaging (or MR imaging) and motion management tools for better targeting of radiation dose to PTVs.
As advancements in imaging technologies progress, we may observe an expansion of applications beyond anatomical changes. For instance, there could be a shift towards incorporating functional imaging results during treatment or other indicators of treatment response—with mid-treatment plan optimization—to create a personalized total dosage for optimal outcomes based on disease and tumor type.
According to Percy Lee, his department at City of Hope in Orange County is taking full advantage of its MRidian. “With a machine like the ViewRay, I look at it like a three-prong machine. You can draw smaller margins (from 4mm to 2mm) and ditch fiducials in the process for prostate SBRT. For tumors that exhibit a large amount of movement, like lower lung, treating with DIBH and cine imaging, the technology intelligently allows you to gate the beam and have confidence in your delivery. And, of course, there’s adaptive,” says Lee.
Shaping the Future
At the moment, in its relative infancy, online ART is a balancing act between embracing the potential and acknowledging the clinical practicalities. In a delicate environment of decreasing reimbursement and value-based care initiatives, it’s imperative that we carefully weigh the pros and cons of adaptive. “Ultimately, I think it will be the standard of care for many sites,” says Price.
Investing in automation, streamlining workflows, and prioritizing data collection are crucial steps to bridge the gap between skepticism and practical adoption. In the meantime, there is plenty of optimism and enthusiasm to drive the field forward. “Online adaptive is here to stay. It’s not for every patient but there is a clear benefit for many indications,” adds Chuong.

Leave a comment