Compliance & Clinical Solutions
Radiation Therapy Billing FAQ: Part One
Billing is an essential function in radiation therapy departments but can be challenging for any clinician. Part 1.
Common Coding Mistakes in Radiation Oncology (And How to Avoid Them)
Radiation oncology coding and billing is nothing short of complex.
It’s a process that requires systematic and structured review of the charge process to validate the necessity of treatment modalities, apply proper coding techniques, catch/prevent errors, ensure billing compliance, and optimize revenue. We’ve found a strong cause and effect relationship tied to quality assurance checks for proper coding that promotes—or hinders—the outcome of the revenue cycle.
At Radformation, we’ve had the unique opportunity to work one-on-one with departments across the country, exploring their billing practices in depth. We’ve gained valuable insights by reviewing the varied approaches of our clinical partners, uncovering many common missteps in their process. It’s our pleasure to identify opportunities for process improvement and provide education and strategies to promote revenue integrity. Below is a compilation of the recommendations we’ve gleaned as a result of our conversations with clinics.
Getting Direct
The written directive outlines the plan of care for radiotherapy, providing a guide for the expected services during a course of radiation. This document is the compass for a patient’s course of treatment and dictates the services needed, preliminary medical necessity, and defined goals. It can also serve as a guide for authorization and coding when well documented.
When reporting 77261-77263 codes represented in the clinical directive documentation, it’s crucial to understand that only one code is applicable for the patient’s entire course of therapy. That’s the case even if multiple treatment sites are present, combined modalities are necessary, or significant changes occur through the entire course of radiotherapy. Almost all questions related to coding and billing require review of this documentation to determine the intent and plans for care. This is the best place to start, because if we can’t get this documentation right, it’s all downhill from here!
Why is Documentation So Important?
The absence of documentation can make it hard to demonstrate that any given service was actually required or ever completed. This can be the most common risk of compliance in all service lines and can lead to poor revenue outcomes for all general and specialty medical services. According to recent data from the Centers for Medicare & Medicaid Services (CMS), it’s obvious that we’ve got work to do as it pertains to documentation.
CMS runs an audit of all its claims each year to estimate the number of improper payments via their Comprehensive Error Rate Testing (CERT) program. Each year, they review a stratified random sample of fee-for-service claims to determine if they were paid properly under Medicare coverage, coding, and payment rules. The 2023 Medicare FFS estimated improper payment rate was a staggering 36% for radiation oncology, representing $330M in improper payments.
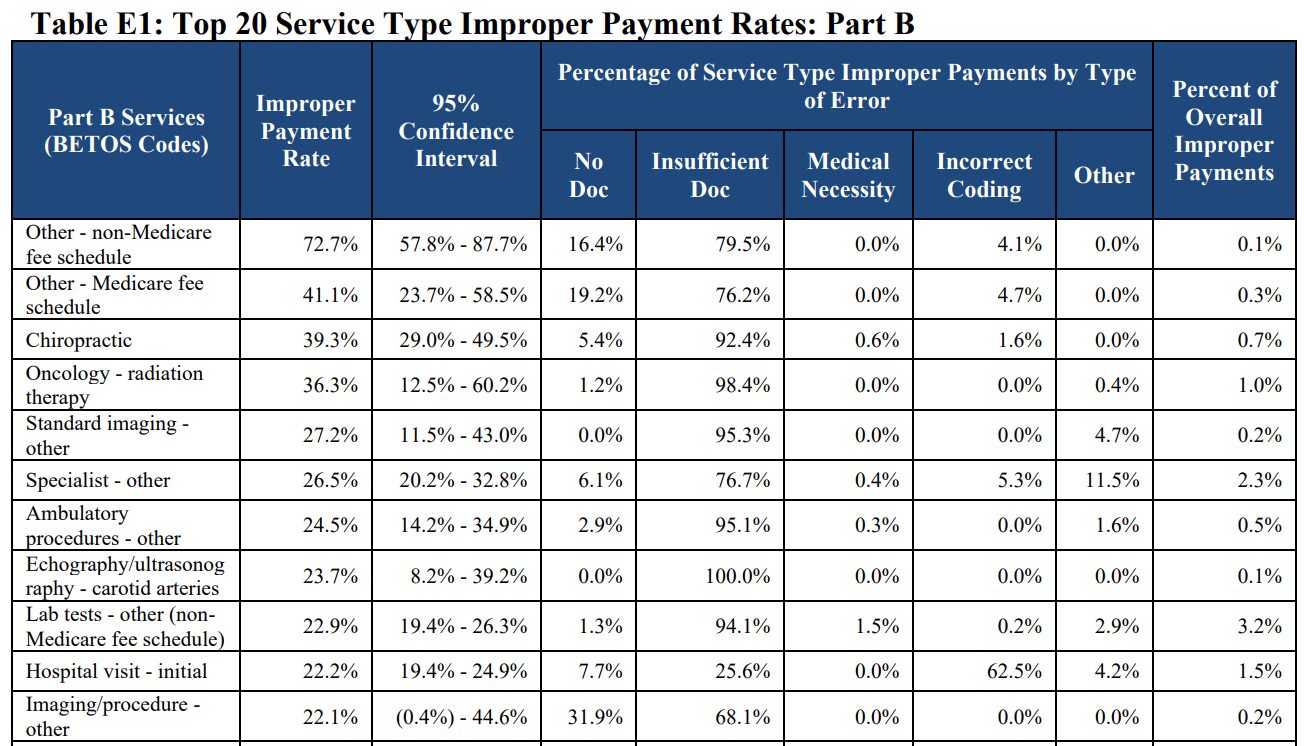 2023 CMS CERT report showing improper payment rates for fee-for-service claims.
2023 CMS CERT report showing improper payment rates for fee-for-service claims.
In our experience, we’ve seen similar issues with documentation misses and errors with the departments we partner with. Whether it’s a missing document, the documentation lacks a physician signature or timestamp, or the proper date of service and supporting information is missing, failing documentation puts facilities at risk of non-compliance and payer revenue recovery. What’s your process for preventing this risk?
The Claim Paid So It Must Be Right!
Is receiving a payment for services a guarantee? The answer is NO!
Payment for services can be reviewed or audited for any reason, at any time. Without consistent claim review to ensure proper coding and billing, you may be at risk even if you’ve already received payment. Like departments, at times even payers make mistakes, and they have teams in place to recoup their payments when this occurs.
Common Mistakes Seen That Can Delay Payment or Lead to Payment Losses:
Given the importance of billing accuracy, what is your facility doing to evaluate their coding and billing processes?

Charge Audits
The best way to prevent errors in billing is to periodically evaluate internal standards on a full episode of care performed by physicians and medical staff. Performing billing audits is crucial for protecting revenue and compliance by identifying coding, billing, and documentation problems before a payer does.
There are several ways to go about this quality assurance for billing, including leveraging the expertise of a third party company or consultant, performing a self-audit (either manually or using software), or securing software or analytics programs to perform an audit. The findings of an audit can validate standard operating procedures, identifying coding mistakes and issues, performing documentation checks, and improving revenue integrity. A comprehensive audit should include a proper evaluation of the following departmental operations:
The outcome of an audit identifies gaps, errors, and risks which are difficult to appreciate from day to day operations. The process reinforces and promotes the accountability of each member of the treatment team, enhances optimal reimbursement, and reduces compliance risks.
Common Coding Flops
Through helping departments perform coding audits with QuickCode, we’ve seen it all. While some errors are unique, we frequently see the same issues crop up at multiple institutions. Here are a few common coding misses and opportunities for improvement:
Individually, These errors may seem small but the effects are huge in clinics everywhere! It is highly recommended for facilities to establish standard operating procedures related to planning processes to include the validation and process for review to prevent these costly misses or errors. Consider these misses when reviewing daily charges, performing month end checks, or auditing the patient’s codes and documentation as part of the final treatment process.
Conclusion
How are you looking at your coding and billing processes in your specialty service lines like Radiation Oncology? What does that look like for comprehensive reviews for end of month efforts or end of treatment audits…perhaps you’re seeing similar issues crop up? Hopefully these insights from our interactions with departments can help you validate your own internal processes to continually improve your practice. If you’re looking for a trusted partner, reach out for a demonstration of QuickCode or request an in-depth ROI analysis.

For your convenience, we’ve also compiled some of our billing tips into a printable PDF. Download the PDF

Leave a comment