Treatment Planning
Treatment Planning FAQ: Acuros XB Dose Reporting Mode
Which dose reporting method for AXB (and other MC-based algorithms) is best for clinical use: dose-to-water or dose-to-medium?
We’re launching our FAQ series with a comparison between Eclipse’s AAA and Acuros.
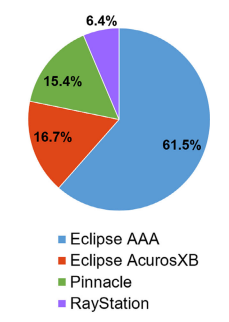
You have two algorithms at your fingertips in Eclipse: Analytical Anisotropic Algorithm (AAA) and Acuros XB (Varian Medical Systems). Which do you choose? More clinics and institutions have added Acuros XB to their arsenal over the last several years, highlighting this important clinical consideration. Acuros is a fundamentally different algorithm based on solving the linear Boltzman transport equation (LBTE), and is heralded for its accuracy. But does it hold up in all clinical scenarios?
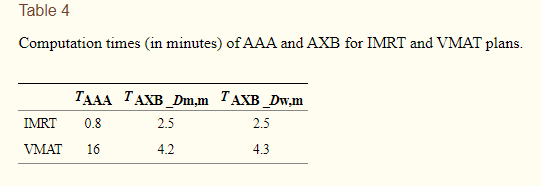
For VMAT calculations, calculation speed is 4x faster than AAA. For plans that require multiple iterations, the time savings stacks up.
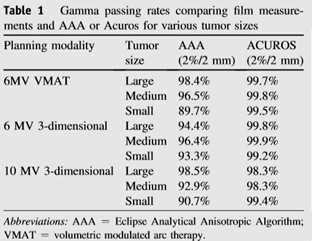
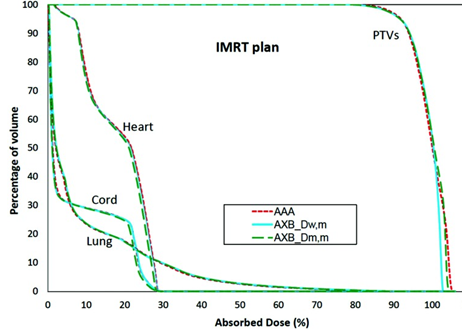
It’s a more accurate treatment model for heterogeneous media, such as bone, lung, and tissue interfaces, according to Yan, et. al. Their study showed that for large lung tumors, AAA dose calculation is accurate (even surpassing the Acuros agreement for 10X), with results depending on the energy; overall however, Acuros calculations show consistently better agreement than AAA. Additionally, Acuros performs better in the presence of air gaps.
Nonetheless, some have voiced concerns about dose reporting Acuros, as the algorithm can display dose by two different approaches: dose to medium (Dm) and dose to water (Dw). While Varian suggests using Dm for patient calculations, others think Dw is better suited to match commissioning data. Suffice it to say this is probably a topic for another blog post.
Plan calculation speed for 3D and IMRT plans is more than 5x faster than Acuros. Also, data suggests AAA shows similar dose calculation accuracy to Acuros XB for homogeneous tissue. For some sites such as breast or abdomen, there isn’t a meaningful clinical difference between the two algorithms.
So…which is better? I’d venture to say most would argue that it depends on the anatomical site and clinical impact. Because it’s broadly more accurate and shows faster VMAT calculation times, perhaps Acuros is better suited for VMAT plans. And for sites that involve variable density (lung, esophagus, etc.), plenty of data suggest Acuros is the best bet. However, for sites where heterogeneity is less of an issue and AAA is shown to agree well with dose measurements, the advantage of faster calculation speed with AAA for 3D and IMRT plans cannot be understated.

Leave a comment