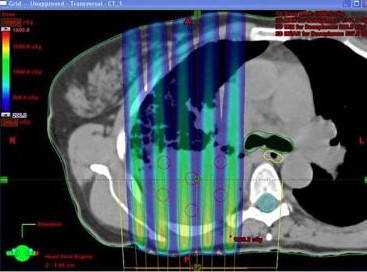
Historically, low-dose shadows were introduced intentionally and were useful in the days of kilovoltage (kV) to partially spare the skin, a major limitation in kilovoltage radiotherapy for deep-seated tumors at the time. GRID therapy differs from conventional radiation therapy in which the targeted dose to the tumor is uniform.
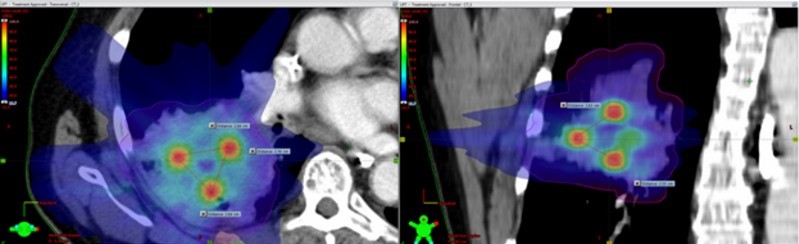
Employed in three dimensions, lattice therapy was designed to modernize GRID therapy and to improve conformality and high doses to surrounding normal tissues. In 3D lattice radiotherapy, the goal is to create small high dose spheres, called vertices, within the tumor and keep lower dose regions closer to the periphery of the tumor in order to spare healthy tissue. These vertices are spaced strategically depending on the tumor size, shape, and location in normal tissue. 3D lattice radiotherapy has been used clinically and has resulted in improved local control, with no increased toxicity.
Investigating the use of 3D lattice radiotherapy on patients with bulky non-small cell lung cancer, Amendola, et al. showed no associated mortality and no increased toxicity in a small cohort of 10 patients that received the lattice therapy as an adjunct to conventional radiation, in which 18Gy at the lattice vertices, central in the tumor, and of 3Gy at the periphery of the tumor. The mean decrease in tumor size following treatment at a median follow-up time of six months was 42%.
A review of SFRT by Billena and Khan explains that the bystander effect is triggered by certain cytokines being expressed or downregulated due to proximity of highly irradiated cells. Vascular damage via endothelial apoptosis can be caused in low dose SFRT regions due to local travel of soluble radiation byproduct. This damage inhibits tumor growth and sustainability. In the absence of high dose there is an anti-tumor response from the immune system that aids in cancerous cell death in the low dose region. It is also possible that this could trigger a more distant abscopal effect.
{kind=link}
{kind=link}
{kind=link}